Preprosthetic care prepares your mouth for a stable, comfortable prosthesis, whether that is a denture, an implant-supported restoration, or another appliance. By reshaping bone and soft tissue, oral pre-prosthetic surgery improves fit, function, and long-term success. Below is what to know about pre-prosthetic surgery, what to expect, how to plan, and why timing matters.
When and Why Pre-Prosthetic Surgery Is Needed
Pre-prosthetic surgery is recommended when oral tissues need to be optimized before placing dentures, partials, or dental implants. The aim is to create a smooth, well-contoured foundation so your prosthesis seats properly, feels comfortable, and stays stable during chewing and speaking. Understanding what to know about pre-prosthetic surgery helps set expectations and supports better outcomes.
Common reasons include preparing for complete or partial dentures, improving the ridge for implant placement, and correcting areas that cause sore spots or instability under a prosthesis. After tooth loss, bone resorption can leave sharp edges, undercuts, or irregular ridges. Soft tissue concerns such as high frenum attachments, shallow vestibules, or mobile tissues can interfere with denture seal and stability or complicate hygiene around implants. In many cases, pre-prosthetic surgery procedures address both bone and soft tissue issues at the same visit.
Timing depends on overall health, healing capacity, and oral hygiene. Medical factors like diabetes control, blood thinners, osteoporosis medications, and tobacco use can influence scheduling and approach. Your clinician will also consider recent extractions, any infections, and the timeline for delivering your prosthesis so healing is complete before final impressions. This planning phase is a key part of oral pre-prosthetic surgery.
Types of Pre-Prosthetic Procedures and What to Expect
Several routine pre-prosthetic surgery procedures may be used alone or in combination to create the best foundation:
Alveoloplasty: Smooths and reshapes the jawbone after extractions or to refine irregular ridges.
Ridge augmentation: Adds bone or bone substitutes where volume is insufficient for implant placement or to improve denture support.
Frenectomy: Releases a tight lip or tongue frenum that can dislodge a denture or cause tissue pull.
Vestibuloplasty: Deepens the space between the lips or cheeks and gums to enhance denture retention and hygiene access.
Most procedures are performed with local anesthesia; oral or IV sedation may be offered for comfort depending on complexity and preference. During preprosthetic surgery, the provider carefully incises and reflects the tissue, contours bone as needed, adjusts soft tissue attachments, and places sutures for optimal healing.
Benefits include improved fit, fewer sore spots, better retention, and more predictable outcomes for implants or dentures. Risks are generally low but can include temporary swelling, bruising, discomfort, bleeding, infection, changes in sensation, or the need for additional procedures if healing or bone volume is limited. As with all pre-prosthetic surgery procedures, individualized assessment guides the safest, most effective plan.
Recovery is typically straightforward. Many patients resume normal activities within 24 to 72 hours, with soft tissue healing in about 2 to 3 weeks. Bone grafts and ridge augmentation may require several months to mature before implant placement or final denture fabrication. Post-operative care usually includes cold compresses for the first 24 hours, prescribed or over-the-counter pain control, saltwater or antimicrobial rinses as directed, a soft diet, and avoiding straws, smoking, and vigorous activity. Keep the area clean with gentle brushing around the surgical site, follow suture care instructions, and attend all follow-up visits after oral pre-prosthetic surgery.
Planning, Outcomes, and Working With Your Dental Team
Successful care starts with a detailed evaluation. Your team will complete a clinical exam, review your medical history, and obtain imaging such as panoramic X-rays or CBCT scans to assess bone height, width, density, sinus position, nerve location, and soft tissue anatomy. Digital models and bite records help plan the surgical approach and coordinate with your future prosthesis, ensuring that preprosthetic steps align with restorative goals.
By correcting ridge irregularities and soft tissue issues, pre-prosthetic surgery improves denture fit and stability, enhances comfort, reduces sore spots, and supports clearer speech and stronger chewing efficiency. For implants, proper ridge preparation can increase primary stability, reduce complications, and improve long-term implant survival and hygiene access. These are core outcomes to consider when reviewing what to know about pre-prosthetic surgery.
Consider asking your oral surgeon or prosthodontist:
Which pre-prosthetic surgery procedures do I need and why?
What are my anesthesia or sedation options?
How long is healing before impressions or implant placement?
What risks or limitations apply in my case?
How will this affect the look, feel, and maintenance of my dentures or implants?
Are there non-surgical alternatives and how do they compare?
If you are considering dentures or implants and want to optimize your outcome, schedule a consultation with a qualified provider to create a tailored plan for oral pre-prosthetic surgery and guide you through each step of preprosthetic care.
So, what is an impacted canine? An impacted canine is a permanent “eye tooth” that doesn’t erupt into the mouth on time or in the correct position. Because upper canines help guide your bite, support facial aesthetics, and protect other teeth during chewing, identifying and treating impaction early is important for long-term oral health. Below is an overview of causes, how an impacted canine is diagnosed, and the orthodontic and surgical treatments commonly used.
What Is an Impacted Tooth?
An impacted tooth is a permanent tooth that fails to fully emerge into its normal spot in the dental arch. Although any tooth can be impacted, an impacted maxillary canine (upper canine) is the second most frequently impacted after wisdom teeth. Lower (mandibular) canine impaction is less common but can still affect function and appearance. If you are wondering what an impacted canine is in practical terms, it is a canine that remains trapped in the jaw or palate and needs guidance or surgical assistance to reach its proper position.
Impaction is different from delayed eruption, in which a tooth is late but still follows a normal path, and from ectopic or partial eruption, where a tooth breaks through in an abnormal direction or location. With impaction, a barrier or an altered path of eruption prevents the tooth from coming in without assistance. This is especially relevant for an impacted maxillary canine, which often deviates toward the palate.
Possible signs include a noticeable delay compared with the opposite side, a baby canine that remains longer than expected, asymmetry in the smile, swelling or tenderness above the canine area, spacing or crowding in the upper front teeth, and occasional pain with biting or chewing. Sometimes there are no symptoms, and the issue is found on routine dental X-rays.
Causes and Risk Factors for Impacted Canines
Multiple factors can increase the likelihood of an impacted canine:
Insufficient space in the upper jaw due to crowding
Unfavorable tooth angulation or a blocked eruption path
Retained primary (baby) canine that doesn’t shed on time
Dental anomalies, such as peg-shaped lateral incisors, that alter normal guidance
Genetic influences can also contribute. A family history of impacted teeth, variations in tooth size or shape, and extra (supernumerary) teeth may disrupt normal eruption. Certain developmental conditions can affect timing and tooth movement, increasing the chance of an impacted maxillary canine.
Environmental and behavioral factors include dental trauma to baby teeth, premature loss of primary teeth that removes natural guidance, and oral habits that influence arch development. Scar tissue, cysts, or other pathology along the eruption path can also interfere and lead to an impacted canine.
Diagnosis and Early Recognition
Early recognition generally starts with a clinical exam. Upper canines typically erupt between ages 11 and 12. If a baby canine is still present beyond this timeframe or there is a clear right–left difference, an orthodontic evaluation is advisable. Additional signs, such as a bulge high in the gum over the canine region or the absence of a palpable canine “bump” by ages 10 to 11, may prompt imaging and referral.
Imaging helps determine the tooth’s position and its relationship to neighboring roots:
Panoramic X-ray: Provides an overview of tooth development, angulation, and obstacles such as extra teeth.
Periapical radiographs: Offer detailed, localized views of the root and surrounding bone.
Cone beam CT (CBCT): Supplies 3D information about exact location and proximity to adjacent roots, aiding precise treatment planning and reducing risks.
Detecting an impacted canine early often allows simpler, more predictable treatment. Creating space and removing impediments before canine roots fully develop can guide the tooth into place, sometimes avoiding impacted canine surgery or later extraction.
Treatment Options: Exposure, Orthodontics, and Surgery
When an impacted canine is favorably positioned, conservative measures may be effective. Your orthodontist may monitor eruption with periodic imaging, extract a retained baby canine to clear the path, and use orthodontic appliances to create or maintain space. In selected cases, timely space creation alone allows the canine to erupt naturally, particularly for an impacted maxillary canine detected early.
If the tooth does not come in on its own, exposure and bonding is a common next step. An oral surgeon or periodontist makes a small opening in the gum (and sometimes bone) to uncover the canine and bonds a tiny bracket or attachment to it. The orthodontist then applies gentle traction using braces or clear aligners to guide the canine into its proper position. Treatment length varies from several months to more than a year, depending on the tooth’s location and response to movement. Typical short-term effects include gum soreness, minor bleeding, and swelling; irritation to adjacent roots is uncommon. Most patients resume normal activities within a day or two, with instructions for hygiene and comfort.
When the canine is severely malpositioned, fused to the bone (ankylosed), or threatens the health of adjacent teeth, surgical removal may be recommended. In these cases, the orthodontist and oral surgeon coordinate a plan to maintain bite function and appearance. Options may include closing the space orthodontically, redistributing space for a future dental implant once growth is complete, or reshaping adjacent teeth to mimic the canine. If exposure and traction are not feasible, impacted canine surgery can involve extraction and careful space management to preserve aesthetics and function.
A team-based approach tailors care to your age, stage of dental development, and smile goals. Whether treatment involves orthodontic traction after exposure or impacted canine surgery, early diagnosis and coordinated planning help protect neighboring teeth, support facial harmony, and achieve a stable bite.
Understanding how insurance covers oral surgery can be confusing because benefits may come from your dental plan, medical plan, or both. Coverage depends on the procedure, why it is needed, and where it is performed. This guide explains how insurance typically works for oral surgery, when medical insurance may apply, what dental insurance usually pays, and how to minimize surprises before treatment. Our aim is to help you make informed decisions about your care and your costs. If you are researching how insurance covers oral surgery, the sections below outline the key factors that influence coverage and out-of-pocket expenses.
What Counts as Oral Surgery and Common Procedures
Oral surgery includes surgical treatment of the mouth, teeth, jaws, and related structures. Common procedures include wisdom tooth extractions, dental implants, bone grafting, corrective jaw (orthognathic) surgery, biopsy of oral lesions, and management of facial trauma or infections. Some procedures may be performed by a general dentist; others require an oral and maxillofacial surgeon.
Routine dental treatment focuses on preventive and basic restorative care, such as cleanings, fillings, and simple extractions. Surgical or medically necessary procedures extend beyond routine care and address impacted teeth, pathology like cysts or tumors, traumatic injuries, or structural problems that affect function, breathing, or overall health.
Oral surgery may take place in a dental office, an oral and maxillofacial surgery clinic, or a hospital or ambulatory surgery center. The setting can influence billing, office-based care is often billed to dental insurance, while hospital-based care may involve medical claims for facility and anesthesia services. However, the clinical indication and complexity, not just the setting, ultimately determine which insurance applies. Knowing how insurance covers oral surgery in different settings can help you anticipate which plan will be billed first.
What Dental Insurance Usually Covers
Most dental plans cover portions of oral surgery when it addresses dental conditions. Typical covered services include simple and surgical extractions (including some wisdom teeth), limited surgical procedures such as minor bone smoothing or soft tissue surgery, and necessary exams and radiographs before and after treatment. Coverage varies by plan; services like implants or bone grafts may be covered, partially covered, or excluded.
Important plan features to review:
Annual maximum: The total amount your plan will pay per calendar or plan year.
Deductible: The amount you pay before coverage begins for certain services.
Waiting periods: Time you must be enrolled before specific services are covered.
Coverage percentages: Many plans classify services as preventive, basic, or major, with different coinsurance levels. For example, a plan might cover 70–80% for basic extractions and 50% for major surgical services, up to the annual maximum.
Using in-network providers can reduce your costs because they accept contracted fees. Out-of-network care may be reimbursed at lower rates and can involve balance billing. Prior authorization (often called a pre-determination) and complete clinical documentation, X-rays, treatment notes, and narratives, can improve reimbursement and provide clearer cost estimates before treatment.
When Medical Insurance May Cover Oral Surgery
Medical insurance may apply when the primary reason for treatment is medical rather than dental. Situations that may qualify include:
Trauma and injuries such as facial fractures or lacerations.
Cancer-related procedures, including biopsies, tumor removal, and reconstruction.
Treatment of pathology with systemic implications, such as cysts or serious infections.
Procedures required due to medical conditions, for example surgery for sleep-disordered breathing or care needed before cancer therapy.
Severe infections or impacted teeth that cause systemic involvement or threaten overall health.
Claims are often influenced by factors such as the clinical intent (treating disease, injury, or dysfunction), the risks to systemic health (like spreading infection or inability to maintain nutrition), the need for hospital or operating room services, and physician or multidisciplinary involvement. When these elements are present, medical plans are more likely to recognize the procedure as a covered medical service.
To assess medical coverage, obtain pre-authorization if your plan requires it, collect relevant medical records (physician notes, imaging, and pathology reports), and submit documentation that connects the oral surgery to a medical diagnosis. A thorough pre-authorization package that includes medical necessity narratives and appropriate diagnostic codes helps establish expectations for coverage and your estimated out-of-pocket costs.
Dental vs. Medical Billing and Claims
Dental and medical claims use different coding systems and forms. Dental claims typically use CDT procedure codes and are submitted on a dental claim form. Medical claims use CPT procedure codes and ICD diagnosis codes, usually submitted on a CMS-1500 or similar medical claim form. Accurate coding and clear documentation of medical necessity help ensure the claim is routed to the correct insurer and processed correctly.
Some cases involve coordination of benefits or dual billing. For instance, a dental plan might cover the tooth extraction, while a medical plan covers anesthesia or facility fees related to a qualifying medical condition. Your care team can help determine the primary payer and whether a secondary plan may cover remaining eligible costs.
To reduce the risk of denials:
Verify network status for all providers and facilities.
Obtain any required pre-authorizations.
Submit complete clinical records, including imaging and narratives.
Follow your plan’s submission rules and timelines.
If a claim is denied, review the explanation of benefits to identify the reason. You can appeal within the plan’s timeframe by providing operative reports, X-rays, pathology results, letters from physicians, and a detailed narrative explaining medical necessity. Many denials are resolved when additional documentation clarifies the diagnosis, complexity, or urgency.
Costs, Financing, and How to Check Your Coverage
Your out-of-pocket costs depend on the procedure, complexity, treatment setting, type of sedation or anesthesia, and the specialists involved. As a general guide, simple extractions may cost a few hundred dollars per tooth, while impacted wisdom teeth removal, bone grafting, or implant placement typically cost more. Hospital-based procedures include separate facility and anesthesia charges, which can increase total costs but may be covered by medical insurance when medically necessary.
Clear estimates before treatment and flexible payment options can make planning easier. Many offices can help you verify benefits, submit pre-determinations, and provide an itemized breakdown of expected costs. Payment options may include in-house payment plans for eligible services and third-party healthcare credit programs, subject to approval.
To confirm your coverage, contact your dental and medical insurers and ask how your benefits apply to the specific procedure. Request a written pre-determination when available and bring your insurance details to your consultation so the team can verify benefits. Consider asking:
Will this procedure be billed to dental insurance, medical insurance, or both?
Are pre-authorization and specific documentation required?
What are my deductibles, coinsurance, and annual maximums?
What percentage does my plan cover for surgical services?
Is the provider and facility in-network?
Are anesthesia and facility fees covered, and at what rate?
What is my estimated out-of-pocket cost?
Understanding how insurance covers oral surgery before you schedule helps you avoid surprises and choose the most cost-effective setting for care.
Quick Reference: Dental vs. Medical Coverage
Scenario
Likely Primary Coverage
Notes
Simple extraction for tooth decay
Dental
Usually covered as basic or major service, subject to annual maximum.
Impacted wisdom teeth with local infection
Dental, possibly Medical
Medical may apply if there is systemic involvement or hospitalization.
Facial trauma with fractures
Medical
Hospital, facility, and anesthesia fees typically billed to medical.
Biopsy or removal of oral lesion
Medical
Often covered when tied to diagnosis and medical necessity.
Dental implant placement
Dental (varies)
Coverage varies widely; some plans exclude implants or grafting.
Orthognathic (corrective jaw) surgery
Medical
Typically requires pre-authorization and documentation of functional impairment.
How a Care Team Can Help
Insurance policies differ, but you do not have to navigate them alone. A knowledgeable team can review your benefits, coordinate any needed pre-authorizations, and provide a transparent estimate before treatment. They can work with both dental and medical insurers and guide you on documentation, coding, and timelines to support a smooth claims process. If a claim is denied, they can help you understand the explanation of benefits and prepare an appeal when appropriate.
If you are considering oral surgery or have been referred for evaluation, schedule a consultation and bring your insurance information. You will get clarity on how insurance covers oral surgery and what to expect financially, so you can move forward with confidence.
Jaw surgery, also called orthognathic surgery, corrects how the upper and lower jaws fit together and how the face functions and appears. Understanding why you may need jaw surgery starts with identifying whether your challenges stem from jaw position rather than tooth alignment alone. If you struggle with chewing, breathing, speaking, chronic jaw pain, or have a noticeable jaw imbalance, surgery may be part of a comprehensive plan to improve your health and confidence. In some cases, double jaw orthognathic surgery is recommended when both the upper and lower jaws need repositioning to achieve a stable, functional bite and enhanced facial harmony.
Overview: What Jaw Surgery Is and Who It Helps
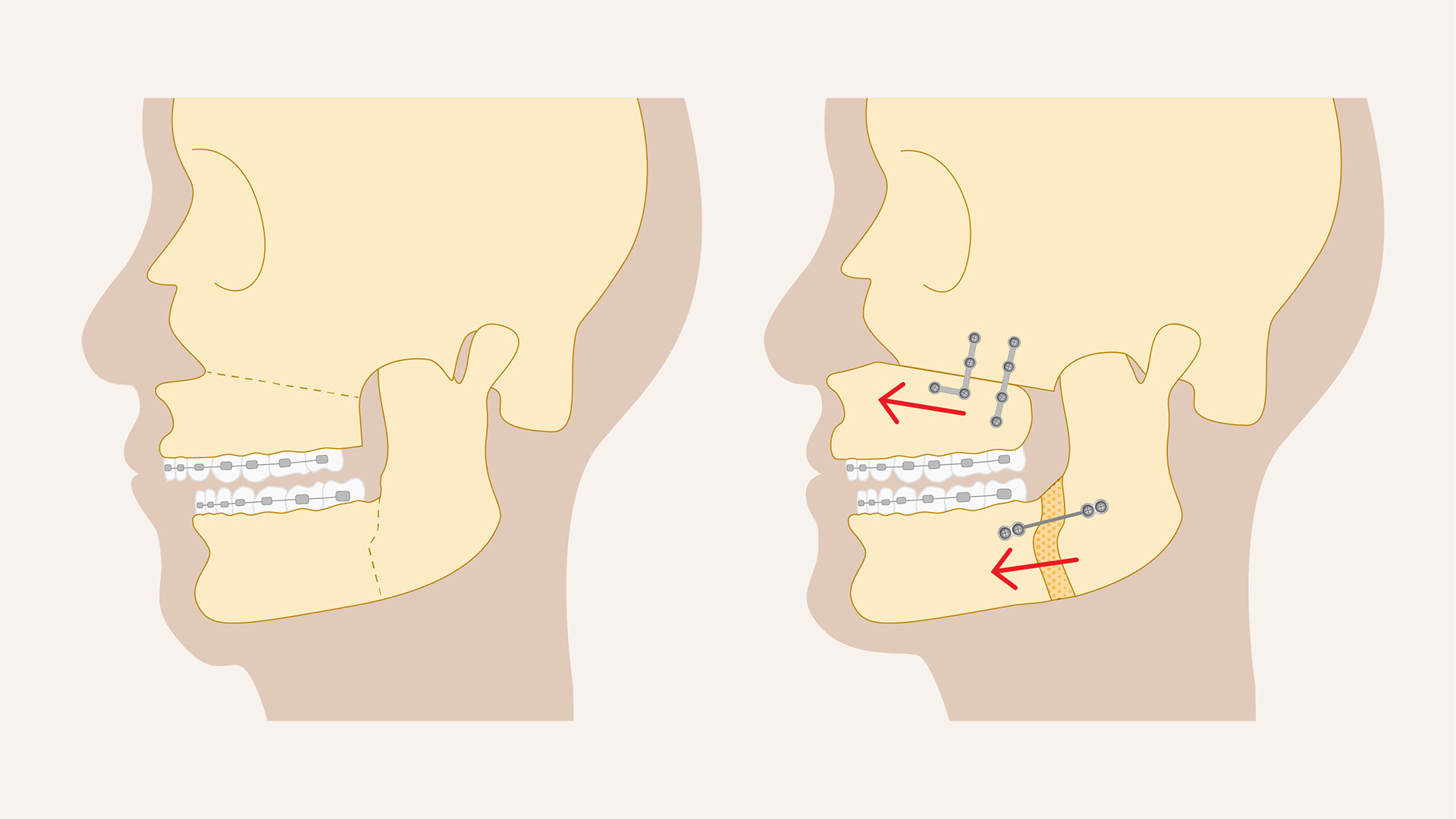
Orthognathic surgery is a corrective procedure performed by an oral and maxillofacial surgeon to reposition the jaws for better function and facial balance. It is often coordinated with orthodontic treatment to align the teeth before and after surgery. Common procedures include maxillary surgery (upper jaw), mandibular surgery (lower jaw), and genioplasty (chin repositioning). These may be performed individually or in combination to create a stable, functional bite and a balanced facial profile. When both jaws are involved, double jaw orthognathic surgery may be the most effective way to correct significant discrepancies.
Patients who benefit from jaw surgery typically have jaw size or position discrepancies that braces or aligners alone cannot correct. Conditions commonly treated include severe overbite or underbite, open bite, crossbite, jaw asymmetry, and concerns related to congenital differences or past facial trauma. Jaw surgery can also be part of treatment for obstructive sleep apnea when airway narrowing relates to jaw position, and it can help patients with temporomandibular joint (TMJ) disorders when structural differences contribute to symptoms. Recognizing why you may need jaw surgery, such as persistent bite problems, airway issues, or facial imbalance, helps determine the best path forward.
Primary goals include improving function so you can chew efficiently, speak clearly, and breathe more easily, while enhancing facial harmony. Many patients experience fewer headaches, less jaw strain, and improved comfort once the jaws and teeth work together properly. Aesthetic improvements are a welcome benefit, but the foundation of treatment is long-term health, stability, and quality of life.
Signs and Symptoms That Suggest You May Need Jaw Surgery
Not every bite issue requires surgery, but certain patterns indicate a skeletal problem rather than a tooth alignment concern alone. Recognizing these signs can help you decide when to seek an evaluation and clarify why you may need jaw surgery instead of orthodontics alone.
Dental and bite indicators: Deep overbite, significant underbite, open bite (front or back teeth do not meet when the jaws are closed), and crossbite (upper teeth sit inside lower teeth). You may notice difficulty chewing, uneven tooth wear, or teeth that fail to meet evenly despite orthodontic care.
Breathing, sleep, and speech clues: Loud snoring, gasping during sleep, or daytime fatigue associated with obstructive sleep apnea may relate to a small or retruded jaw. Chronic mouth breathing, especially with a narrow upper jaw, and speech challenges linked to jaw position (such as difficulty forming certain sounds) may reflect an underlying skeletal imbalance.
Pain and functional concerns: Chronic jaw pain, TMJ clicking or locking, frequent headaches, difficulty swallowing, or a history of facial trauma can indicate that the jaw structure is out of balance. Noticeable facial asymmetry, one side of the jaw appearing longer, wider, or set back, often signals a skeletal difference that may require combined orthodontic and surgical care.
Evaluation and Qualification: How We Determine If Surgery Is Right for You
Determining whether you need jaw surgery begins with a comprehensive evaluation. The process clarifies why you may need jaw surgery and whether a single-jaw procedure or double jaw orthognathic surgery is most appropriate. The assessment starts with a dental exam and bite analysis to see how your teeth come together. Imaging is essential: cephalometric X-rays and CBCT scans provide detailed views of jaw position, airway space, and joint health. Clinical photos document facial symmetry and profile, and when sleep issues are suspected, a sleep study may be recommended to assess for obstructive sleep apnea.
Orthodontic and medical preparation are key to successful outcomes. Many patients wear braces or clear aligners before surgery to align the teeth within each jaw so they fit correctly after repositioning. Timing matters: for growing patients, treatment typically waits until growth is complete to ensure stability, while adults can proceed once dental and periodontal health are optimized. Your care may involve a team that includes an orthodontist, oral and maxillofacial surgeon, primary care physician, and sometimes a sleep specialist or speech therapist. Medical clearances help confirm that anesthesia and surgery are safe for you.
Clear criteria guide recommendations. If your bite discrepancy is primarily dental, non-surgical options such as braces, aligners, elastics, and bite correction appliances may be sufficient. Surgery is recommended when the problem is skeletal, meaning the jaws themselves are misaligned, or when airway obstruction, facial asymmetry, or functional issues cannot be corrected with orthodontics alone. In complex cases, double jaw orthognathic surgery can correct vertical, transverse, and front-to-back discrepancies in a single coordinated procedure. Risks, benefits, and alternatives are reviewed so you can make an informed decision aligned with your goals.
What to Expect: Procedure, Risks, Recovery, and Outcomes
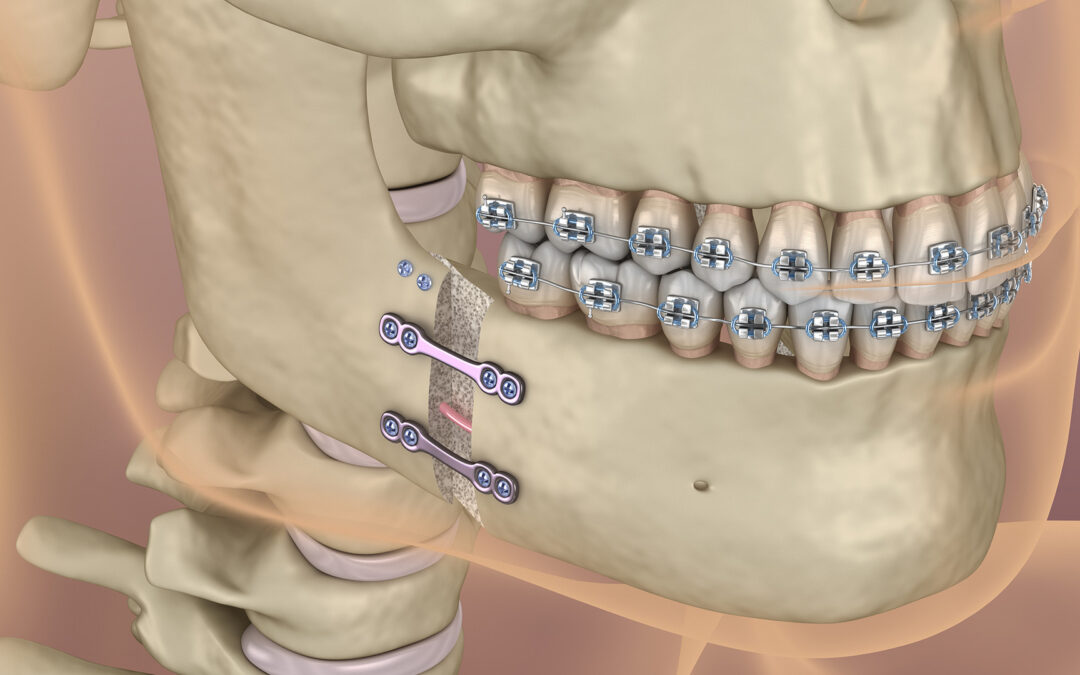
Jaw surgery is performed in a hospital or accredited surgical center under general anesthesia. The surgeon repositions the jawbones using precise cuts made inside the mouth to avoid visible facial scars. Plates and screws are typically used to stabilize the new position during healing, and elastics may guide the bite. Most patients go home the same day or stay one night, depending on the complexity of the procedure and overall health. When both jaws require repositioning to correct the bite and airway, double jaw orthognathic surgery may be recommended and follows similar surgical principles.
As with any operation, there are risks. Potential complications include swelling, bruising, temporary numbness of the lips or chin, bleeding, infection, and bite changes that may require adjustment. Less common risks include nerve injury with prolonged numbness, joint discomfort, relapse of jaw position, and the need for revision surgery. The benefits can be significant: improved bite efficiency, clearer speech, reduced jaw strain and headaches, better breathing and sleep quality for appropriate candidates, and enhanced facial balance. Setting realistic expectations about what surgery can and cannot change is essential and helps define why you may need jaw surgery as part of a long-term health plan.
Recovery is gradual and well supported:
Swelling peaks in the first week and improves noticeably over two to three weeks.
Pain is typically managed with prescribed medications, then over-the-counter options.
A soft or liquid diet is followed initially, progressing to more solid foods over four to six weeks as healing allows.
Good oral hygiene, including gentle rinsing and careful brushing, helps prevent infection.
Orthodontic follow-up continues after surgery to fine-tune the bite, and guiding elastics may be used for a period.
Physical activity is limited at first. Most patients return to school or desk work in one to two weeks and to more strenuous activities once cleared by the surgeon.
Long-term results are designed to be stable and functional. With proper orthodontic finishing and retention, you can expect lasting improvements in chewing, speech, comfort, and facial aesthetics. Regular check-ins with your orthodontist and surgeon help protect your investment in your health and smile.
Common Reasons You May Need Jaw Surgery
Concern
How Surgery Helps
Severe overbite or underbite
Repositions the jaws so upper and lower teeth meet correctly for a stable, efficient bite. In complex cases, double jaw orthognathic surgery addresses both jaws to optimize function and balance.
Open bite
Closes gaps between front or back teeth so they contact properly for chewing and speech.
Crossbite
Expands or repositions the upper or lower jaw to align arches and improve function.
Jaw asymmetry
Balances uneven jaw growth to improve facial symmetry and bite alignment.
Obstructive sleep apnea (anatomy-related)
Advances the jaws to open the airway, which can reduce snoring and apnea events. Double jaw orthognathic surgery may be used to enlarge the airway when both jaws contribute to narrowing.
TMJ problems with structural causes
Corrects jaw position to reduce strain on the joints and associated symptoms.
Post-traumatic or congenital differences
Restores function and balance after injury or developmental variations.
Getting Started
If you notice signs that jaw surgery might help, the first step is a consultation with an orthodontist and an oral and maxillofacial surgeon. They will review your concerns, complete a thorough exam, and create a coordinated plan that may include orthodontic preparation, a single-jaw procedure, or double jaw orthognathic surgery. Many patients appreciate having a clear timeline for orthodontic preparation, surgery, and finishing touches, along with transparent information about recovery and costs.
Your smile, comfort, and overall health matter. Schedule a visit with a qualified team to learn whether jaw surgery is right for you, better understand why you may need jaw surgery, and explore a treatment plan that fits your life.
Orthognathic (corrective jaw) surgery repositions the jaws to improve bite function, facial balance, and airway health. Understanding orthognathic surgery expectations before, during, and after surgery helps you prepare confidently and recover smoothly. This guide covers candidacy, planning and imaging, the hospital experience, recovery milestones, and long-term outcomes so you can make informed decisions with your care team.
Understanding Orthognathic Surgery
Orthognathic surgery is performed by an oral and maxillofacial surgeon to reposition the upper jaw (maxilla), lower jaw (mandible), or both. It is recommended when jaw size or position cannot be corrected with braces alone. Good candidates are teens and adults with near-complete or completed growth who have functional concerns such as difficulty chewing, speaking, or breathing, or noticeable facial imbalance.
Conditions commonly treated include underbite, overbite, open bite, crossbite, facial asymmetry, a recessed chin or midface, and obstructive sleep apnea related to jaw position. In some cases, it may help address bite issues associated with TMJ disorders when coordinated with appropriate therapies.
The goals are to create a stable, healthy bite, enhance facial harmony, and improve breathing. Benefits often include easier chewing and speaking, improved smile aesthetics, better airway function (especially during sleep), reduced tooth wear, and long-term oral health stability when combined with orthodontic treatment.
Preparing for Surgery: Preoperative Expectations
Most patients complete a period of pre-surgical orthodontics to position the teeth optimally on each jaw. Your orthodontist and surgeon will coordinate the sequence of tooth movement and surgical timing. This collaboration helps ensure a stable final bite and supports your aesthetic goals while aligning with realistic orthognathic surgery expectations.
Your evaluation may include a physical exam, dental scans or impressions, X-rays, CBCT imaging, photographs, and digital models. Many teams use virtual surgical planning with 3D-printed guides or splints to enhance precision. You will review the plan, including risks, benefits, and alternatives, and provide informed consent after your questions are answered.
Plan ahead at home and work. Most people need one to two weeks away from school or desk work, with a longer timeline for physically demanding jobs. Arrange help with transportation, meals, and errands for the first several days. Prepare recovery supplies such as cold packs, a blender, protein shakes, soft foods, lip balm, a humidifier, prescribed medications, a water flosser, and wax or silicone for braces. Create a comfortable resting area with extra pillows to keep your head elevated. Confirm insurance authorization and complete any necessary time-off paperwork.
The Day of Surgery and Hospital Experience
On the day of surgery, you will check in, review the treatment plan, and meet the anesthesia team. Most procedures are performed under general anesthesia. After you are asleep, the surgeon makes incisions inside the mouth, repositions the jawbones, and secures them with small plates and screws. Incisions are closed with dissolvable sutures, and elastics may be placed to guide your new bite.
Procedure time varies by complexity. One-jaw surgery often takes two to four hours, while double jaw orthognathic surgery may take four to six hours. Afterward, you will recover in a monitored area where your breathing, heart rate, and comfort are observed closely. Some patients go home the same day; others stay one night for observation.
Upon waking, expect facial swelling, a sense of fullness or congestion, and temporary numbness in the lips or cheeks. Your bite will feel different. Pain is typically manageable with prescribed medications and cold therapy. Nurses will help you start fluids and review how to use elastics, oral rinses, and cold compresses. The first 24 hours focus on rest, hydration, cold packs, head elevation, and gentle oral care with prescribed rinses.
Recovery Timeline and Common Postoperative Issues
Recovery is a gradual process. While everyone heals at a different pace, these milestones are common:
First week: Swelling and bruising usually peak around days two to three, then begin to subside. Stick to liquids and very soft foods. Keep your head elevated and use cold packs as directed. Most people can speak softly, move around the house, and do light activities.
Weeks 2–6: Transition from liquids to soft foods with your surgeon’s approval. Swelling gradually decreases and energy improves. You will attend orthodontic and surgical follow-ups to adjust elastics and monitor healing.
Months 3–6: Most swelling resolves, strength returns, and normal chewing gradually resumes as cleared by your surgeon. This phase is particularly meaningful for those who underwent double jaw orthognathic surgery, as muscular adaptation continues.
One year: Final refinement of your bite and smile with orthodontic finishing and retainer wear. Results continue to mature as tissues settle.
Common postoperative symptoms include swelling, bruising, nasal congestion (especially after upper jaw surgery), mild bleeding from the nose or mouth, and temporary numbness or tingling in the lips or cheeks. Nerve sensation often improves over weeks to months. Pain is typically moderate and well controlled with medications and consistent icing and elevation.
Know the warning signs that require prompt attention: a fever over 101.5°F that does not respond to medication, increasing facial pain or swelling after initial improvement, foul-tasting drainage, difficulty breathing, inability to keep fluids down, uncontrolled bleeding, or irritation over hardware. Contact your surgeon immediately if any of these occur.
Your team will schedule regular orthodontic visits to guide your bite into its final position. Plan a gradual return to normal eating: clear liquids, full liquids, purees, then soft foods such as eggs, pasta, fish, and cooked vegetables before moving back to regular textures. Avoid hard, crunchy, or chewy foods until you are cleared. Light walking is encouraged early. More strenuous exercise and contact sports should wait until your surgeon confirms bone healing, typically six to eight weeks or longer depending on the procedure.
Setting Realistic Orthognathic Surgery Expectations
Clear communication with your care team helps align orthognathic surgery expectations with your goals. Discuss functional priorities like chewing and airway, as well as aesthetic preferences. Ask about the anticipated amount of swelling, how long elastics or splints will be used, and expected timelines for returning to work, school, and exercise. Patients undergoing double jaw orthognathic surgery may experience slightly longer swelling and dietary restrictions, but many also report more comprehensive improvements in facial balance and bite stability.
It is normal to have questions about sensation changes, including numbness or tingling, especially in the lower lip and chin. Most changes improve over time, though some residual numbness can persist. Your surgeon will explain risks, how nerves are protected, and what you can do to support recovery.
Long-Term Outcomes and Patient Expectations
Final results unfold as swelling resolves and orthodontic finishing is completed. Most patients achieve a more stable bite, improved chewing efficiency, enhanced facial balance, and, when indicated, better sleep and breathing. Scars are hidden inside the mouth. The small plates and screws usually remain in place permanently unless there is a specific reason to remove them.
Maintaining oral health supports long-term stability. Brush gently with a soft toothbrush and use a water flosser around braces and surgical areas once approved. Wear elastics and retainers exactly as prescribed. Keep all follow-up appointments so your team can monitor healing, adjust your bite, and address concerns early. Contact your surgeon promptly if you notice new or worsening pain, bite changes, signs of infection, or if elastics or splints come loose.
Emotional adjustment is part of the process. Swelling can temporarily change your appearance, and numbness can feel unfamiliar. Many patients find that taking progress photos, following care instructions, and leaning on supportive friends and family helps. If you feel anxious or discouraged, ask your team about support groups or counseling resources.
Tips for a smooth recovery:
Stay hydrated and well nourished with protein-rich soft foods.
Sleep with your head elevated for the first couple of weeks.
Use cold compresses initially, then warm compresses as directed.
Avoid tobacco and vaping to support healing.
Follow medication schedules and activity guidelines closely.
With careful planning, consistent follow-up, and teamwork between your orthodontist and surgeon, most patients experience long-lasting functional and aesthetic improvements from orthognathic surgery. Understanding orthognathic surgery expectations ahead of time, particularly for double jaw orthognathic surgery, can make the journey smoother and the results more predictable.
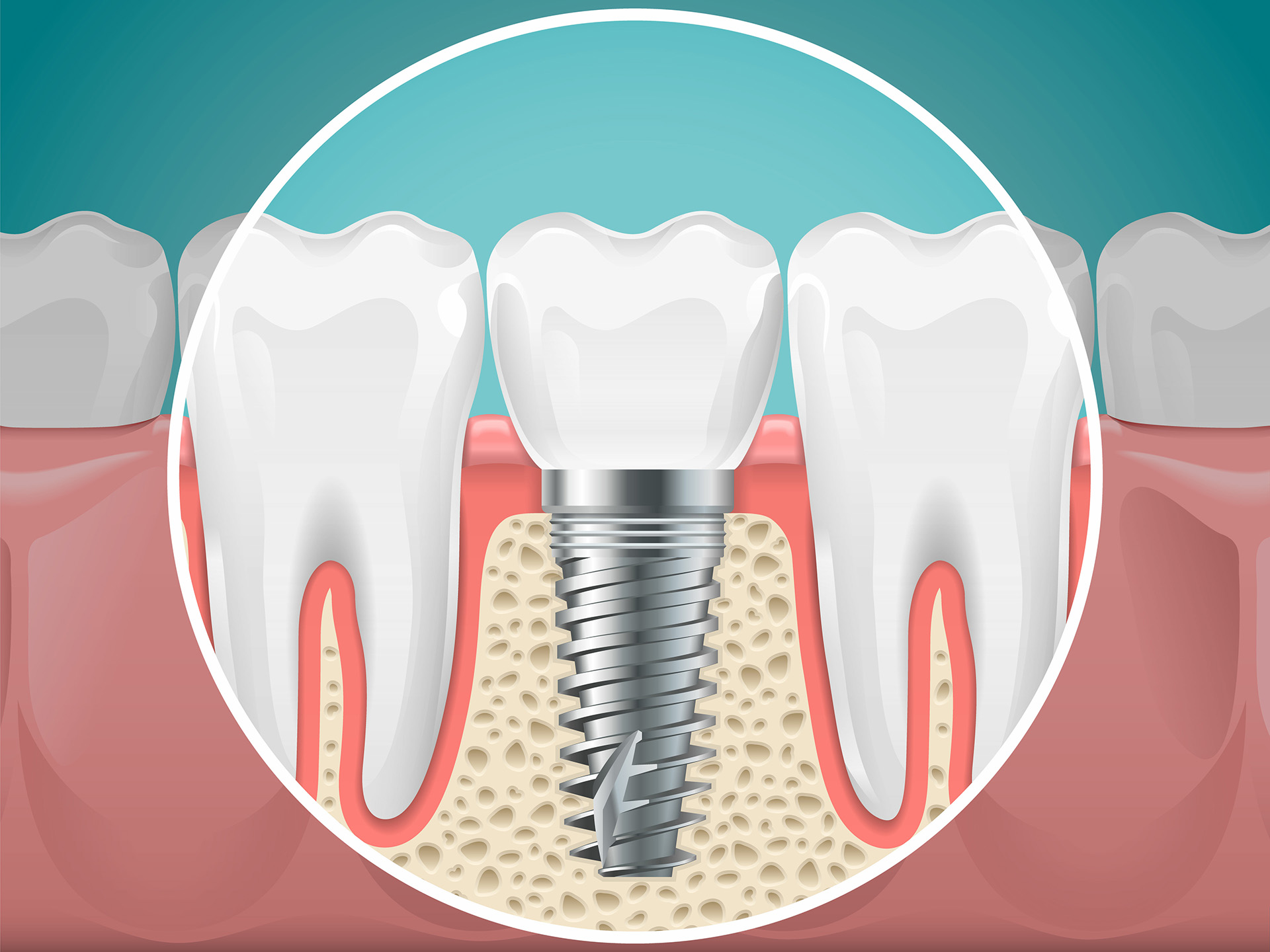
Dental implants have an excellent long-term success rate, but complications can occur, especially without careful planning and maintenance. Knowing the most common problems with dental implants, how they start, what to watch for, and how they are treated, helps you protect your investment and oral health. Below, we outline early and late complications with dental implants, nerve and sinus concerns, patient risk factors, key warning signs, and proven solutions to keep implants healthy for the long term. We also address frequently reported side effects of dental implants and tooth implantation side effects so you know what is expected versus what needs attention.
Early Surgical and Healing Complications
During the first few days to weeks after placement, the implant site is actively healing. Mild soreness and swelling are typical tooth implantation side effects and usually resolve quickly. Early complications with dental implants usually relate to infection control, bleeding, and establishing stable osseointegration (fusion between implant and bone). Being aware of early dental implants problems allows you to act promptly if symptoms worsen.
Post-operative infection arises when bacteria enter the surgical site before the tissue seals. Contributing factors include inadequate plaque control, smoking, unmanaged systemic conditions, and contamination during home care. Signs include increasing pain after initial improvement, swelling that worsens after day three, warmth, redness, bad taste, or discharge. Prompt evaluation allows for targeted antibiotics, irrigation, and local care to prevent progression.
Bleeding and swelling are common immediately after surgery. Some swelling and oozing are expected side effects of dental implants, but persistent bleeding beyond 24 hours or rapidly expanding swelling needs attention. Firm bite pressure on gauze, cold compresses, rest, and avoiding strenuous activity usually control mild issues. In some cases, medication adjustments or additional suturing may be required.
Poor osseointegration occurs when the implant does not fuse with bone. Risk factors include early overloading (chewing hard foods too soon), infection, insufficient primary stability, smoking, and systemic health problems. Patients may notice persistent discomfort or a lack of functional improvement, while clinicians may detect mobility at follow-up.
Wound dehiscence refers to reopening of the incision or soft tissue over the implant. Causes include suture tension, thin or fragile tissue, trauma, and poor oral hygiene. Management may involve protective dressings, refined home care, additional suturing, or soft tissue grafting to ensure coverage.
Early implant mobility is a warning sign. Any movement in the first weeks typically indicates inadequate stability or failed integration. Your clinician may reduce loading (remove temporary crowns), adjust your bite, or remove and replace the implant after healing, depending on timing and severity.
Late-Onset Implant Problems
After initial healing, implants function much like natural teeth. However, complications with dental implants can develop months or years later, often involving inflammation around the implant, mechanical issues, or gradual changes to bone and gum tissues. These dental implants problems are usually manageable when caught early.
Peri-implantitis and mucositis: Peri-implant mucositis is gum inflammation without bone loss. If unmanaged, it can progress to peri-implantitis, a chronic infection with bone loss around the implant. Risk factors include poor oral hygiene, smoking, a history of periodontal disease, and inconsistent professional maintenance. Symptoms may include bleeding on brushing, swelling, persistent bad taste, pus, or deepening pockets around the implant.
Mechanical loosening and fractures: Late mobility often stems from prosthetic component issues such as a loose or fractured abutment screw, cracked porcelain, chipped crowns, or worn attachments. You may notice clicking, movement while chewing, or a change in your bite. Early evaluation can prevent minor problems from becoming structural failures.
Bone loss and gum recession can develop gradually. Contributing factors include peri-implantitis, thin gum biotype, aggressive brushing, poorly contoured restorations, or biomechanical overload from grinding. Signs include longer-looking crowns, visible metal margins, or food impaction. Timely intervention, such as bite adjustments, soft tissue grafting, and improved plaque control, can preserve stability.
Nerve, Sinus, and Soft-Tissue Considerations
Nerve-related issues are more common in the lower jaw, where the inferior alveolar and mental nerves run. Symptoms include numbness, tingling, burning, or shooting pain in the lip, chin, or tongue. Prevention depends on precise imaging, meticulous planning, and guided surgery to maintain safe distances from nerve pathways. If symptoms occur, immediate evaluation is essential. Early steps, such as relieving pressure, removing an offending implant, or prescribing medications, can improve the chances of recovery.
Sinus complications may occur with upper jaw implants near the maxillary sinus. Signs include persistent one-sided nasal congestion, sinus pressure, a whistling sound or air passage through the implant site, drainage, or recurrent sinus infections. Prevention includes pre-surgical imaging, sinus lift or grafting when needed, and atraumatic surgical techniques. If problems develop, management may involve antibiotics, decongestants, closing any sinus communication, or referral to an ENT specialist for persistent cases.
Soft-tissue irritation around implants can present as redness, tenderness, or bleeding when brushing. Causes include plaque buildup, ill-contoured restorations, or rough material surfaces. Mucosal overgrowth can trap debris and fuel inflammation; contour refinement or adjusting the crown often resolves the issue. True titanium allergies are rare, but sensitivities to certain components or surface contaminants can occur. Evaluation may include allergy history and clinical testing, and in select cases, considering alternative materials such as zirconia.
Patient and Lifestyle Factors That Increase Risk
Identifying and managing patient-specific risks before and after surgery significantly improves outcomes. Daily habits, systemic health, bone quality, and bite forces all influence long-term success and the likelihood of common problems with dental implants.
Oral hygiene: Inadequate plaque control triggers inflammation and peri-implant disease. Consistent home care, twice-daily brushing, cleaning between teeth with floss or interdental brushes, and using antimicrobial rinses as directed, reduces risk.
Tobacco use: Smoking and other tobacco products impair blood flow, slow healing, and increase infection and bone loss. Quitting before surgery and staying tobacco-free afterward is one of the best ways to protect an implant.
Systemic conditions: Diabetes, osteoporosis, and immune disorders can affect healing and infection control. Well-controlled diabetes has significantly better outcomes than uncontrolled disease. Some medications, including bisphosphonates or other antiresorptives, immunosuppressants, and certain chemotherapy agents, require careful planning with your physician. Always share a complete medical and medication history with your dental team.
Bone quality and volume: Insufficient density or volume may require bone grafting or sinus augmentation to achieve stability and long-term support.
Bruxism and clenching: Excessive forces from grinding can loosen screws, crack porcelain, or contribute to bone loss. Nightguards or occlusal splints, bite adjustments, and stress management help protect implants and natural teeth.
Signs, Symptoms, and When to Seek Help
Early recognition leads to simpler, more successful treatment. Pay attention to changes, even minor ones, and reach out promptly. Distinguish expected tooth implantation side effects like mild soreness from warning signs that indicate complications with dental implants.
Common warning signs
Pain that persists or worsens after the first few days post-surgery
Swelling that does not subside, redness, or warmth
Bleeding on brushing, pus, or an unpleasant taste
Mobility of the implant or crown, or clicking sensations
Bite changes or a crown that feels loose
Numbness or tingling of the lip, chin, or tongue
Sinus pressure, congestion, or drainage after upper jaw surgery
Timing matters
Early (first 2–6 weeks): Persistent pain, swelling, or early mobility often point to infection, inadequate stability, or wound problems.
Late (months to years): Bleeding on brushing, bad taste, gum recession, or intermittent swelling suggest peri-implant mucositis or peri-implantitis. Sudden clicking or movement typically indicates a loose component or screw.
Contact your dental team right away if you experience ongoing pain beyond a few days, persistent swelling, fever, pus, numbness or tingling, bleeding that will not stop, sinus symptoms after upper jaw surgery, or any mobility in the implant or crown. Most dental implants problems are easier to resolve when addressed early, and your provider can triage by phone to determine if urgent in-office care is needed.
Treatment Options, Prevention, and Long-Term Care
Effective care starts with an accurate diagnosis. Your provider will evaluate the implant, surrounding gums, bone levels, and all prosthetic components to determine whether the issue is inflammatory, mechanical, or both. Treatment plans often combine non-surgical therapy with surgical or restorative solutions for best results. Clear guidance helps separate normal side effects of dental implants from treatable complications with dental implants.
Non-surgical treatments
Targeted antibiotics when infection is present
Antiseptic rinses such as chlorhexidine
Professional debridement to remove plaque and calculus from implant surfaces
Bite adjustments to reduce excessive forces
For mechanical issues, tightening or replacing screws, re-cementing crowns, or repairing chipped porcelain
Surgical interventions
Flap surgery to access and decontaminate implant surfaces
Removal of a failing implant when necessary, with planning for future replacement
Maintenance and prevention
Maintenance is the foundation of long-term success and the best defense against common problems with dental implants. Schedule regular professional cleanings and exams based on your risk level, often every three to four months for higher-risk patients. At home, brush twice daily with a soft-bristled brush, clean between teeth and around the implant crown with floss or interdental brushes, and use water flossers when helpful. For grinders, a custom nightguard can protect both implants and opposing teeth. Address minor chips or looseness promptly to prevent larger problems.
If an implant fails
Your dentist will determine whether the implant can be salvaged. Early problems may respond to thorough decontamination and bone or soft tissue grafting. If removal is required, options include immediate replacement in select cases, delayed replacement after healing, or alternative prosthetic solutions such as bridges or partial dentures. Prognosis depends on the cause of failure, bone quality, and how well risk factors are controlled. Many patients achieve successful replacement implants after corrective treatment and improved maintenance.
With careful planning, excellent home care, and consistent professional follow-up, most dental implants problems are preventable or manageable. If you notice any changes or have concerns about your implant, contact your dental team for a personalized assessment and care plan.
Quick Reference: Common Implant Problems and Solutions
Issue
Typical Signs
Contributing Factors
Common Solutions
Early infection
Increasing pain, swelling, redness, discharge
Plaque accumulation, smoking, poor hygiene
Antibiotics, irrigation, local care, improved home care
Immediate evaluation, pressure relief, possible removal, meds
Sinus complications
Congestion, drainage, whistling sound
Sinus membrane breach, infection
Antibiotics, decongestants, closure, ENT referral if persistent
Remember: while some side effects of dental implants such as transient soreness and swelling are expected, persistent or worsening symptoms point to complications with dental implants that deserve prompt care. Understanding the common problems with dental implants equips you to take preventive steps and seek timely treatment if needed.








{kind=link}